
Radical Orchiectomy
While scrotal ultrasound and serum tumor markers (beta-human chorionic gonadotropin, alpha-fetoprotein, and lactate dehydrogenase) are the first steps in the diagnosis of a testis cancer, the diagnosis is not confirmed until an orchiectomy (surgical removal of the testicle) is performed. The standard of care for the removal and treatment of testis cancer is a radical inguinal orchiectomy. This is the most common operation performed for testis cancer worldwide. However, as our understanding of this disease and surgical technique has improved, testis-sparing surgery or partial orchiectomy has become an option for some patients.
Rationale
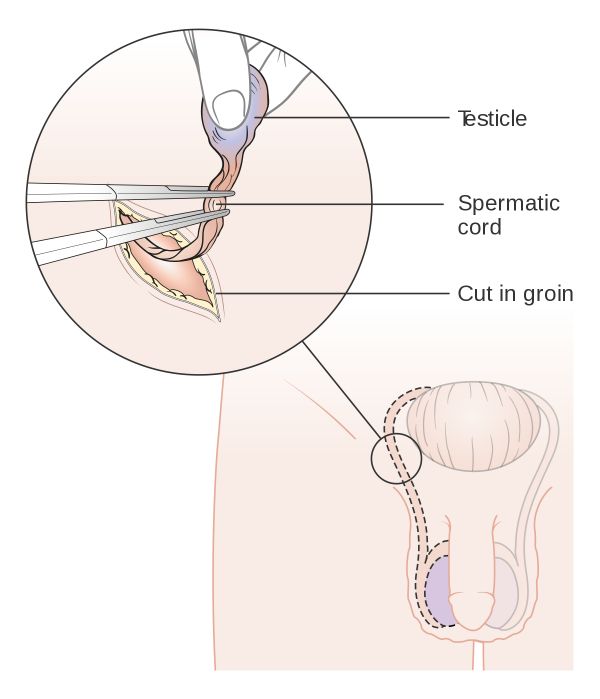
This surgery involves removing the testicle and spermatic cord where it exits the body to identify and likely treat the majority of cancers localized to the testis. As a male fetus develops, the testes develop near the fetal kidneys. As the fetus grows, the testicles separate from the kidneys and, at about the eighth month of pregnancy, the testicles exit the body wall to rest in the scrotum (this is why premature infants have a higher likelihood of having undescended testicles). Therefore the blood supply, lymphatic drainage and nerves to the testicle originate near the kidney on that side.
Once these structures exit the body through the internal inguinal ring, they fuse with muscles of the body wall to form the spermatic cord. To correctly stage and prevent any cancer from spreading, the spermatic cord must be taken as high toward or inside the body as possible — hence the incision in the groin rather than the scrotum.
For men whose cancer has spread from the testicle and who have metastatic testis cancer (elsewhere in the body) or in the lymph nodes of the retroperitoneum, radical orchiectomy is an important first step in the diagnosis and management of disease. Knowing the type of cancer may help guide chemotherapy or radiation treatments.
Surgery
The surgery can be performed under general or local anesthetic. An approximately 5–10-centimeter incision is made in the groin, just above the pubic tubercle (pubic bone) near the inguinal ligament. This incision facilitates access to both the testicle and the inguinal canal. The incision is carried down to the external oblique fascia (the outermost layer of the body wall). The external oblique creates a tunnel through which the spermatic cord travels — a hernia can form when there is weakness in these layers of the body wall.
Once the external oblique fascia is identified, the cord can then be identified exiting the external spermatic ring. The testicle can then be “delivered” from the scrotum. To deliver the testicle, the scrotum can be inverted until the testicle is visible, facilitating dissection of the testicle from its scrotal contents.
Once the testicle and spermatic cord are entirely free from the inguinal canal, the testicle can be removed. Care should be taken to close the external oblique fascia to the level of the external ring to prevent future hernia.
Complications
The biggest risk of a radical orchiectomy is hematoma (or bleeding into the scrotum). It is very common for the scrotum to be bruised, swollen and tender for two to four weeks after surgery. However, a large, purple-appearing scrotum can indicate a hematoma. Hematoma can be prevented with a compressive dressing, tight-fitting undergarments and/or ice packs.
Ilioinguinal nerve injury can occur if the nerve is damaged during dissection of the spermatic cord. This is more common in men who underwent prior inguinal surgery (usually for an undescended testicle or hernia repair) and can occur during dissection or be inadvertently trapped in the closure of the external oblique fascia. The deficit is often decreased sensation to the medial thigh, scrotum or base of the penis. It is often transient, but can take several weeks or months to improve.
Inguinal hernia can occur if the external oblique fascia is not closed properly or if the closure breaks down. It is important to minimize strenuous activities for two to four weeks to prevent development of a hernia.
Testicular Prosthesis
Prostheses should be offered to all men undergoing orchiectomy. Not all men want a prosthesis — it is a personal decision. The prosthesis should be measured in the operating room with the patient asleep. The goal should be to match the remaining testicle in size, taking into account a cancerous testicle can be larger or smaller than normal, and the scrotal skin will make a prosthesis look larger once implanted.
Risks
Risks and complications should be discussed with an individual pre-operatively. Risks and complications for inguinal orchiectomy include scrotal hematoma (accumulation of blood in the scrotum), infection, post-operative pain (60% initially, 1.8% one year after), phantom testis syndrome (pain in the kidney as a result from trauma from the testicle), reduced fertility, and with the more rare complications being inguinal hernia, ilioinguinal nerve injury, tumor spillage, and hypogonadism.
Effects
Unilateral orchiectomy results in decreased sperm count but does not reduce testosterone levels. Bilateral orchiectomy causes infertility and greatly reduced testosterone levels. This can lead to side effects including loss of sexual interest, erectile dysfunction, hot flashes, breast enlargement (gynecomastia), weight gain, loss of muscle mass, and osteoporosis. It has been discovered that some individuals with a history of prostate cancer who had bilateral orchiectomy had effects on their new bone production, resulting in increased risk of bone fractures due to testosterone deficiency after the procedure.
Bilateral orchiectomy also reduces the use of exogenous medications for transgender women; the reduction in testosterone eliminates the need for testosterone-blocking medications and can contribute to feminizing features such as breast enlargement.
Psychosocial Effects
The loss of one or both testicles from orchiectomy can have severe implications in a male’s identity and self-image surrounding masculinity, such that it can lead to an individual having thoughts of hopelessness, inadequacy, and loss. Among testicular cancer survivors who have lost a testicle, there are feelings of shame and loss, which are more evident in young and single men than older and non-single men. As many as one third of individuals who will undergo orchiectomy are not offered the option of having a testicular prosthesis. Data shows that simply offering testicular prosthesis to individuals undergoing orchioectomy is psychologically beneficial. While some individuals do not mind losing a testicle, studies have shown that there is a change in body image in testicular cancer survivors who have undergone orchiectomy and an improvement in body image in 50-60% of individuals who undergo testicular prosthesis placement. One year after testicular prosthesis placement, there are reports of increase in self-esteem and psychological well-being during sexual activity in a study that followed up on post-orchiectomy individuals including adolescents. On the other hand, there is a current debate whether children undergoing orchiectomy should be offered testicular prosthesis to be inserted at the time of orchiectomy procedure.